
Your surgery > During surgery
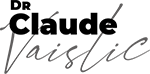
The heart arteries, called coronary arteries, may be narrowed or clogged by calcium or cholesterol deposits. This disease, known as atherosclerosis, is not heart-specific; it can affect any of the body’s arteries. It is caused by smoking, high blood pressure, diabetes, stress, and genetic predisposition.
Coronary arteries narrowed or clogged by arteriosclerosis are unable to pump enough blood to the heart during physical exertion, causing chest pain known as angina. In extreme cases, the artery becomes blocked, leading to myocardial infarction – a heart attack.
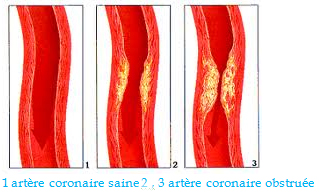
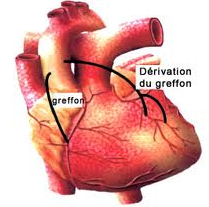
As its name suggests, coronary bypass surgery bypasses the narrowed passages to improve the blood supply upstream from the blockage. It can be performed on any coronary artery of sufficient diameter. Bypasses are most commonly performed on the anterior interventricular artery, the circumflex artery, and the right coronary artery.

Coronary bypass involves grafting a section of a blood vessel, called a conduit, from elsewhere in the body, to supply blood upstream from the occluded arteries. The conduit must be easy to harvest, and neither too large nor too small. It also must be an accessory artery, to prevent causing any tissue damage.
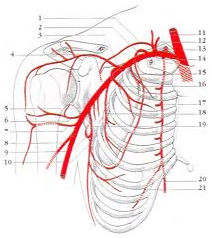
The internal thoracic artery (sometimes called the internal mammary artery), found under the chest wall, is the most suitable blood vessel for coronary artery bypass grafts. Since there is a left and a right internal thoracic artery, at least two coronary grafts may be harvested from this arterial system.
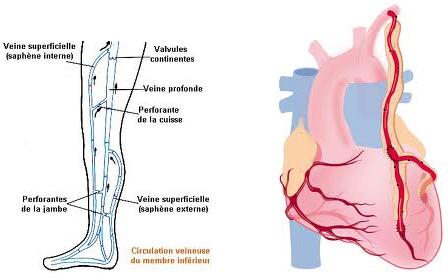
The great saphenous vein, located in the legs, may be harvested for other grafts.
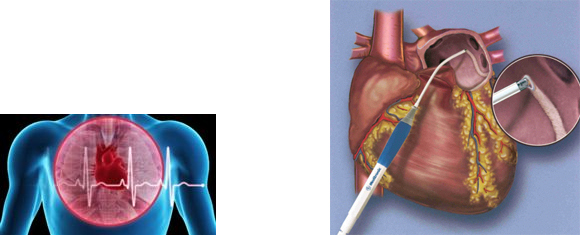
The internal thoracic artery (ITA) is severed from the chest wall without touching its origin on the sub-clavian artery. The ITA is then attached, or « anastomosed », to the coronary artery beyond the occluded section.
The saphenous vein is harvested from the leg. One end is attached to the coronary artery beyond the blockage or narrowing, and the other end is attached to the aorta. The surgeon therefore does not touch the damaged section of the coronary artery. The surgeon sutures the bypass on either end of the affected area using very fine instruments and thread, and magnification devices called loupes.
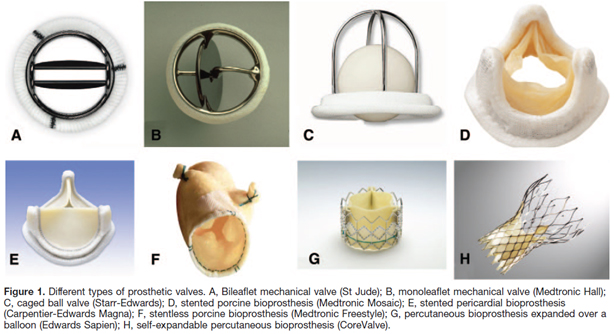
Mechanical valves are made from pyrolytic carbon and last indefinitely, but require lifelong treatment with blood thinners (anticoagulants). They are most often used in patients under age 65.
Tissue valves are taken from animals, and can deteriorate after 10 to 15 years. No blood thinner is required. They are most often used in patients over age 65.
All of these artificial heart valves require excellent oral hygiene to prevent any mouth germs from entering the bloodstream and affixing to the implanted valve, causing inflammation known as endocarditis.
The aortic valve lying at the exit of a patient’s left ventricle may hinder blood flow if it has become fibrotic or calcified. This disease is known as aortic valve stenosis. If the valve keeps blood from being properly pumped out, it must be replaced by an artificial valve which may take the form of a mechanical valve (made of pyrolytic carbon) or a tissue valve harvested from an animal (bioprosthesis).

Sometimes the aorta above the aortic valve is dilated, with a risk of rupture. Ascending aorta surgery is performed to replace the aortic valve and wall with a Dacron tube containing an artificial Bentall valve. The coronary arteries are re-implanted in this tube. In some cases, the aortic valve can be kept during this surgery.

The mitral valve between the left atrium and left ventricle can deteriorate, leading to valve leakage, known as incompetence or regurgitation, or to stenosis. Very often, surgery can repair this valve so it can be kept. However, sometimes the lesions are too extensive and the valve must be replaced by a mechanical or tissue valve.

The heart has an autonomous rhythm that originates in one source in the right atrium (sinoatrial node) and travels down to the ventricle. When the atria are dilated, the heartbeat can originate from several ectopic triggers at once, becoming irregular and chaotic. This is known as atrial fibrillation. When this happens, the heart cannot do its job properly. Heart surgery can be performed to attempt to correct this heartbeat irregularity. It involves creating a pattern of lesions on the atrium walls (using radiofrequency or ultrasound) to block abnormal electrical impulses and re-establish the normal sinoatrial rhythm.
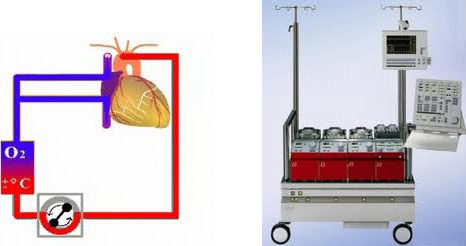
During heart surgery, a form of extracorporeal circulation, known as cardiopulmonary bypass (CPB), can be required to take over the functions of the heart and lungs. A heart-lung machine oxygenates the blood and continues to pump it throughout the body.
Cardiopulmonary bypass is compulsory during valve surgery, since the heart must be opened. It is also preferable during coronary surgery, since the suturing of the coronary arteries is painstaking work, and best performed on a heart that is not beating. It is sometimes possible to attach artery grafts to a beating heart without the use of a heart-lung machine. Called off-pump surgery, this technique requires special conditions.